As ever the headline only tells part of the story.
RNA vaccines seem to produce very different antibody levels
Results raise questions about correlation between protection and antibody levels.

arstechnica.com
Here’s the related paper.
Comparison of SARS-CoV-2 Antibody Response Following Vaccination With BNT162b2 and mRNA-1273
The SARS-CoV-2 messenger RNA (mRNA) vaccines BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna) have each shown more than 90% efficacy in preventing COVID-19 illness
1,
2but, to our knowledge, humoral immune responses have not been compared directly.
Methods
Health care workers at a tertiary care center (Ziekenhuis Oost-Limburg, Belgium) who were scheduled for vaccination with 2 doses of either mRNA-1273 or BNT162b2 were invited to participate in this prospective cohort. Serologic testing was performed prior to vaccination as well as 6 to 10 weeks after the second dose (between April 27 and May 20, 2021). Total immunoglobulin levels to the receptor-binding domain of the SARS-CoV-2 spike protein were measured with an anti–SARS-CoV-2 S enzyme immunoassay (Elecsys, Roche Diagnostics International Ltd). After vaccination, antibodies against the SARS-CoV-2 nucleocapsid protein were determined. Previous infection was defined as anti-nucleocapsid positivity at any point, anti-spike positivity before vaccination, and/or a history of positive polymerase chain reaction results on nasopharyngeal swab.
Antibody levels were compared after the second dose of each vaccine for the entire cohort; for those previously infected vs uninfected; and by age group (<35, 35-55, and >55 years) among previously uninfected individuals, using the
ttest after log10 transformation. Correlation between age and log10-transformed antibody levels was assessed with Pearson correlation. To adjust for confounding, a multiple linear regression was fitted with inclusion of age, sex, previous infection, and time between vaccination and serologic testing. All tests were 2-sided with statistical significance set at α = .05. Analyses were performed using RStudio (version 1.2.1335). This study was approved by the local institutional review board; participants provided written informed consent.
Results
Of 2499 health care workers who received 2 doses of SARS-CoV-2 mRNA vaccines, 1647 participated in this study. A total of 688 were vaccinated with mRNA-1273 (mean age, 43.2 years; 76.7% women; 21.8% previously infected with SARS-CoV-2), and 959 with BNT162b2 (mean age, 44.7 years; 84.9% women; 13.2% previously infected).
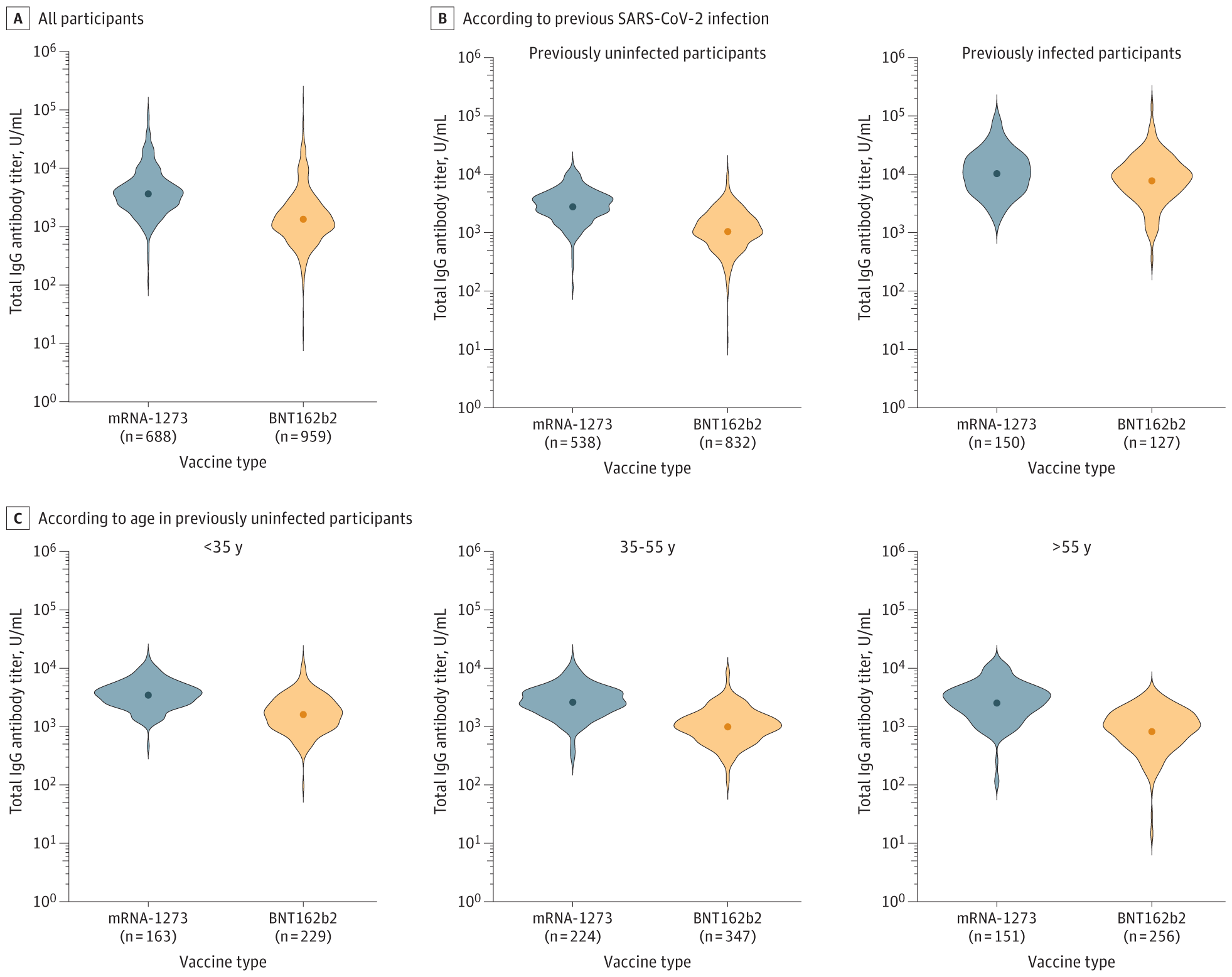
Higher antibody titers were observed in participants vaccinated with 2 doses of mRNA-1273 compared with those vaccinated with BNT162b2 (geometric mean titer [GMT], 3836 U/mL [95% CI, 3586-4104] vs 1444 U/mL [95% CI, 1350-1544];
P < .001) (
Figure, A).
Previously infected participants had higher antibody titers (GMT, 9461 U/mL [95% CI, 8494-10 539]) compared with previously uninfected participants (GMT, 1613 U/mL [95% CI, 1539-1690]) (
P < .001). In both groups, those vaccinated with mRNA-1273 had higher antibody titers compared with those vaccinated with BNT162b2 (previously uninfected: GMT, 2881 U/mL [95% CI, 2721-3051] vs 1108 U/mL [95% CI, 1049-1170];
P < .001; previously infected: GMT, 10 708 U/mL [95% CI, 9311-12 315] vs 8174 U/mL [95% CI, 6923-9649];
P = .01). The difference in antibody levels according to previous infection was higher than the difference between the 2 mRNA vaccines (
Figure, B and
Table).
Antibody levels negatively correlated with age in previously uninfected participants (correlation coefficient, −0.22;
P < .001), being highest among those younger than 35 years. Across all age categories, previously uninfected participants vaccinated with mRNA-1273 had higher antibody titers compared with those vaccinated with BNT162b2 (
P < .001 for all comparisons;
Figure, C).
The type of mRNA vaccine remained independently associated with the log-transformed antibody titer in a multiple linear regression (
P < .001,
Table).
This study compares the immune responses to the BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna) COVID-19 vaccines in health care workers in Belgium.

jamanetwork.com


 www.bbc.com
www.bbc.com


 www.telegraph.co.uk
www.telegraph.co.uk



 inews.co.uk
inews.co.uk

 www.hollywoodreporter.com
www.hollywoodreporter.com
www.manxradio.com

 www.cbsnews.com
www.cbsnews.com








 www.rnz.co.nz
www.rnz.co.nz

 www.independent.co.uk
www.independent.co.uk


 www.nature.com
www.nature.com
